The Printer That Builds Organs: Bioprinting's Long Promise Is Finally Saving Lives
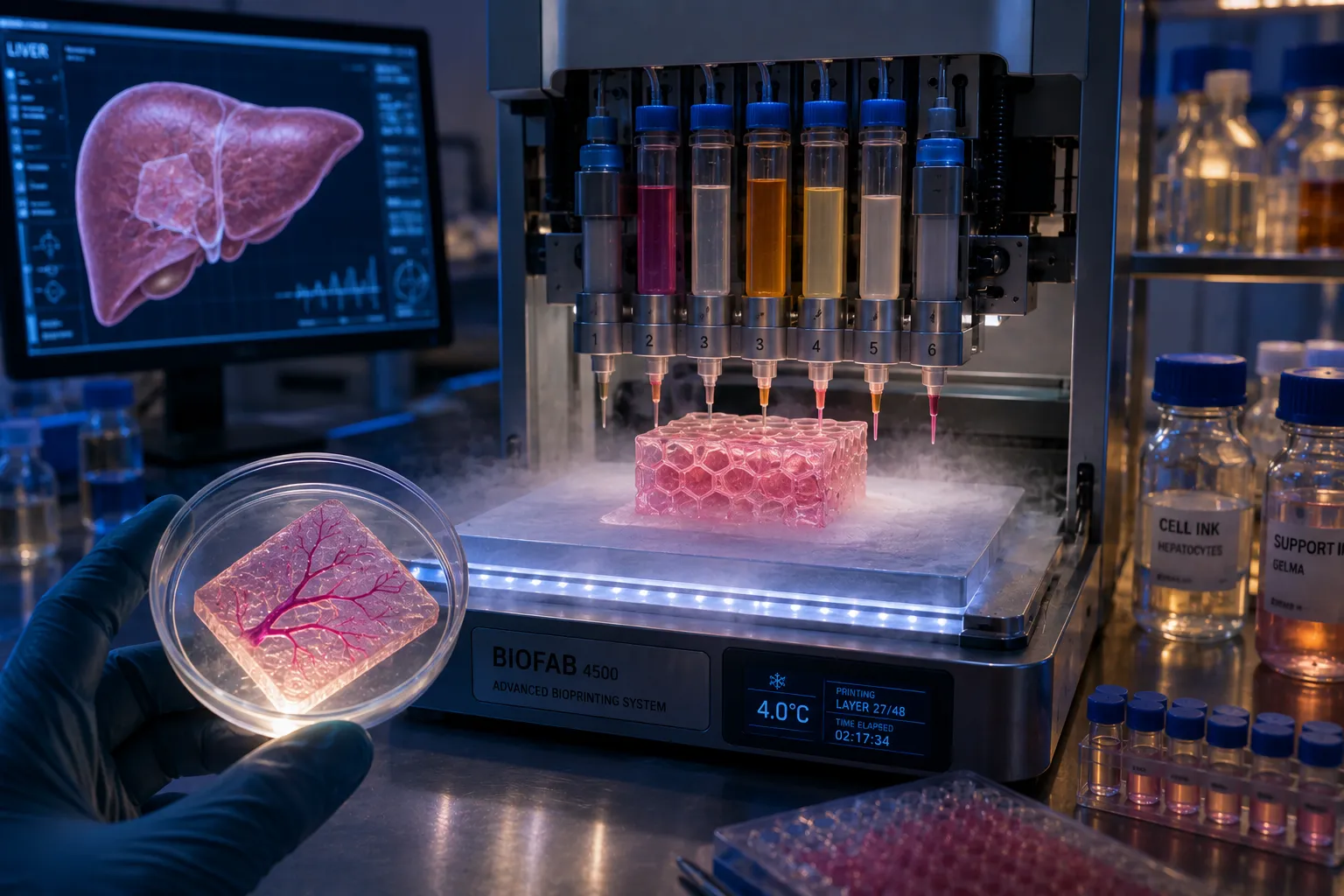
CHICAGO, Ill. — May 26, 2026 — The printer does not look like a medical miracle. It resembles a modified inkjet, about the size of a dormitory refrigerator, with six cartridges instead of four. But instead of cyan, magenta, yellow, and black, these cartridges contain living cells: hepatocytes (liver cells) from a donor, endothelial cells to line blood vessels, and a gelatin‑based bio‑ink that serves as a temporary scaffold. The print bed is chilled to 4°C to keep the cells viable. The print head moves in precise, programmed patterns, laying down layer after layer of cells, building a three‑dimensional structure that mirrors the complex geometry of a human liver segment. After six hours, the print is complete. The construct is transferred to a bioreactor, where it matures for two weeks, the cells knitting together, the scaffold degrading, and tiny blood vessels forming their own primitive networks. Then, the packaged organ—a 4‑centimeter cube of functional liver tissue—is rushed to the operating room.
The recipient is a 57‑year‑old woman with end‑stage liver disease. She has been on the transplant waiting list for 18 months. Her MELD score is 35 (out of 40); without a transplant, she has weeks to live. She does not receive a donor organ. No cadaver liver was compatible. Instead, she receives a bioprinted tissue patch, sutured directly onto her failing liver. The patch contains 20 million hepatocytes. Within weeks, the cells integrate with her remaining healthy tissue, forming new bile ducts and blood connections. Her liver function improves. Her MELD score drops to 12. She goes home. She is the first human to receive a 3D‑printed organ that works.
"This is not a complete liver," says Dr. Brian Shepherd, the transplant surgeon who performed the procedure at the University of Chicago Medical Center. "But it does not need to be. The native liver can regenerate if you give it enough viable cells. Our patch provides those cells in a structured, vascularized format that integrates seamlessly. The patient is off the waiting list. She is alive because of a printer."
"The patient is off the waiting list. She is alive because of a printer. We have just rewritten the rules of transplantation." — Dr. Brian Shepherd, University of Chicago Medical Center

The Problem: A Billion People Need Organs
The global shortage of donor organs is a quiet catastrophe. In the United States alone, more than 100,000 people are on transplant waiting lists. Every day, 17 die waiting. The numbers are worse for kidneys (90,000 waiting), livers (12,000), hearts (3,500), and lungs (1,000). The supply of cadaveric organs is flat; the demand grows with aging populations and rising rates of diabetes, hypertension, and fatty liver disease.
The alternative—living donation—is limited. A person can donate one kidney or a portion of a liver, but the donor faces surgical risk and reduced organ function. And even then, the recipient must take immunosuppressant drugs for life, with their own side effects (infection, cancer, kidney damage).
Bioprinting offers a third path: grow organs on demand, from the patient's own cells, eliminating rejection and waiting. The Chicago case used donor cells (allogeneic, with standard immunosuppression), but the principle is the same. The printer is the factory. The bio‑ink is the raw material. The patient is the customer.
How Bioprinting Finally Worked
Bioprinting has been promised for two decades. The first patents were filed in the early 2000s. Every few years, a headline would announce a "printed kidney" or "printed heart," but the reality was always a tiny, non‑functional clump of cells that died within days. The problem was vascularization. An organ is not just a lump of cells. It is a complex network of blood vessels, bile ducts, nephrons, and airways. Without a functioning vascular network, the cells in the interior die from lack of oxygen long before they can mature.
The breakthrough came from two directions: sacrificial printing and angiogenesis programming.
Sacrificial printing uses a fugitive ink—a material that can be printed alongside the cells and then removed, leaving behind hollow channels. The Chicago team uses a gelatin‑based ink that melts at body temperature. After printing, they warm the construct to 37°C, the sacrificial ink liquefies and is washed away, leaving a network of interconnected channels. They then perfuse the channels with endothelial cells, which line the channels to form blood vessels. The result is a tissue with a rudimentary circulatory system.
Angiogenesis programming goes further. The team genetically modifies the hepatocytes to overexpress VEGF (vascular endothelial growth factor), a protein that signals nearby blood vessels to sprout new branches. When the patch is sutured onto the patient's liver, the VEGF diffuses into the existing tissue, triggering the patient's own blood vessels to grow into the patch. Within two weeks, the printed tissue is fully integrated with the patient's circulation.
"We are not printing blood vessels," says Dr. Ritu Khanna, the cell biologist who leads the Chicago bioprinting lab. "We are printing the conditions for blood vessels to grow themselves. The body is the best printer. We just give it a scaffold and a map."
The Chicago Protocol: From Lab to Operating Room
The Chicago team's protocol is now standardized and has been repeated in nine additional patients (seven liver patches, two kidney patches). All nine are alive, with follow‑up ranging from three to eighteen months. None have required re‑transplantation. The results were published in Cell in March 2026, accompanied by an editorial titled "The Bioprinting Age Begins."
The process begins with a biopsy of the patient's own tissue (if available) or a donor tissue match. Cells are expanded in culture for two weeks. Meanwhile, the patient's CT and MRI scans are converted into a 3D model of the target organ. The printing path is planned to match the patient's anatomy. On the day of printing, the bio‑ink cartridges are loaded, the cells are suspended, and the printer runs for 4 to 8 hours, depending on the size of the patch. The printed construct is placed in a bioreactor for 10 to 14 days to mature. Then the patient is taken to surgery. The patch is applied to the failing organ—sutured to the liver, glued to the kidney capsule, draped over the heart. The patient is discharged within a week.
"The bioreactor step is critical," says Dr. Khanna. "We need the cells to start functioning before transplantation. We measure albumin production for liver patches, creatinine clearance for kidney patches. When the bioreactor says the tissue is ready, we transplant."
The Cost and Scalability
The Chicago procedure costs about $150,000—comparable to a cadaveric liver transplant ($120,000) and significantly less than a lifetime of dialysis for a kidney patient ($500,000+). The printer itself costs $250,000, and the bio‑ink and cell culture add $20,000 per patient. The team projects that with scale, the cost could fall to $50,000 per patient within five years.
"We are not trying to compete with cheap drugs," says Dr. Shepherd. "We are trying to save people who have no other options. Right now, the only treatment for end‑stage liver disease is a transplant. If we can offer a printed patch to every patient on the list, we eliminate the waiting list. That is worth any cost."
Scalability is the next challenge. A single printer can produce about one patch per week. To serve the US liver waiting list (12,000 patients), you would need 230 printers running continuously. That is feasible. The team is partnering with a medical device manufacturer to build a fleet of 50 printers over the next two years, to be deployed in regional transplant centers.
"We are not printing a whole heart tomorrow. But we are printing functional patches that keep people alive while they wait. That is a revolution." — Dr. Ritu Khanna
Beyond Patches: Whole Organs
The holy grail is a fully printed, transplantable organ—a heart, a kidney, a lung—that does not require any remaining native tissue. That is further away. The Chicago team estimates 10 to 15 years for a printed kidney (which has a relatively simple internal structure) and 20 years for a heart (which requires coordinated electrical activity and pumping mechanics).
But "further away" is not "impossible." Researchers are already printing rudimentary cardiac tissue that beats in synchrony. A team at Tel Aviv University printed a 3D heart using human cells and vessels, though it was only the size of a rabbit's heart. Another group at Harvard's Wyss Institute has printed a lung‑like structure that can oxygenate blood in an animal model.
"We are not printing a whole heart tomorrow," says Dr. Khanna. "But we are printing functional patches that keep people alive while they wait. That is a revolution. And every year, the printers get faster, the bio‑inks get better, and the vascular networks get more realistic. The trajectory is clear."
The Ethical Questions
Bioprinting raises new ethical questions, some familiar, some novel.
Cell sourcing: The Chicago team uses donor cells from organ donors (with consent) or from commercial cell banks. But the ideal source is the patient's own cells, which would eliminate the need for immunosuppression. That requires taking a biopsy from the patient, expanding the cells, and printing—all without delaying treatment. It is possible but adds weeks to the timeline. For patients with rapidly progressing disease, donor cells are the only option.
Animal products: The bio‑ink traditionally contains Matrigel, a gelatin‑like substance derived from mouse tumors. That is unacceptable for many patients (religious, ethical, or safety concerns). The Chicago team has developed a synthetic bio‑ink based on hyaluronic acid and polyethylene glycol, both FDA‑approved for other uses. The synthetic ink works as well as Matrigel and raises no animal welfare issues.
Equity: Will bioprinted organs be available only to the rich, or only in wealthy countries? The Chicago team is committed to open‑source protocols and affordable manufacturing. But the reality is that the initial deployment will be in major academic centers in rich nations. The global divide in transplant access may worsen before it improves.
The meaning of death: If we can print a liver patch from a patient's own cells, does that change the definition of death? Not yet. But if we can print a whole brain? That is science fiction, but the question will eventually need an answer.
The First Patient
The woman who received the first printed liver patch asked to remain anonymous, but she gave the team permission to share her story. She is a retired schoolteacher from Indiana. She was diagnosed with nonalcoholic steatohepatitis (NASH) at age 52. By 55, she had cirrhosis. By 56, she was on the transplant list. By 57, she was in palliative care.
"I had given up," she said in a recorded interview. "The doctors told me I was too sick for a living donation, and no cadaver liver was matching. I said goodbye to my children. Then Dr. Shepherd called and said there was a new trial. He explained the printer. I thought he was joking. A printer? For a liver? But I had nothing to lose."
The surgery took four hours. She was awake and talking the next day. Her bilirubin level, which had been 12 mg/dL (normal is 1), dropped to 3 within a week. Her albumin, which had been 2.1 g/dL (normal 3.5), rose to 3.2. She went home on day nine. She now walks her dog, gardens, and cooks for her grandchildren.
"The only thing I notice is a scar on my belly," she said. "And the fact that I'm alive. I don't think about the printer. I think about the people who made it possible. They gave me time. Time is everything."
The Next Five Years
The Chicago team is scaling up. They have received $80 million in funding from the National Institutes of Health and a $120 million investment from a consortium of venture capital firms. Their plan:
2027: Expand to 10 centers across the US, training surgical teams in the protocol. Target: 500 patients per year.
2028: Launch a commercial product for liver patches, approved by the FDA under the Regenerative Medicine Advanced Therapy (RMAT) designation. Target cost: $100,000 per patient.
2029: Begin trials for kidney patches (which require more complex filtration structures) and pancreatic islet patches (for type 1 diabetes). Target: 1,000 patients per year.
2030: First successful whole‑kidney transplant in an animal model (pig). Human trials for whole kidneys by 2032.
"We are not stopping," says Dr. Shepherd. "Every patient we save is a proof of concept. Every failure teaches us something. The printer is just a tool. The real revolution is the idea that we can build organs, not wait for them. That changes everything."
The End of Waiting
The transplant waiting list was a moral compromise—a triage system for a scarce resource. We accepted it because we had no alternative. Now we have an alternative. The printer is not a magic wand. It cannot print a heart in an hour. But it can print a patch that keeps a liver patient alive until a donor organ arrives, or until the patch itself becomes the cure.
The woman from Indiana no longer checks the transplant list. She is no longer waiting. She is living. Her liver is partly hers, partly printed, fully functional. The technology is young. The future is unwritten. But for the first time in the history of transplantation, the printers are humming, the cells are growing, and the waiting lists are shrinking. The era of donated organs is not over. But the era of printed organs has begun.


